
The QDIS-7: using one scale to measure the disease-specific quality-of-life impact of different medical conditions

Summary of main findings
Despite the many differences in content and recall period among the five scales (Supplementary Table S2), the correlations between QDIS-7 scores and legacy-scales scores were substantial (Table 1). That is consistent with the presence of a large common underlying disease-specific QOL-impact factor. Coefficient alpha values for the four QDIS-7 scores indicate that they were highly reliable, and the QDIS-7’s homogeneity allows reliance on a single summary disease-specific score for each condition despite the diversity of QOL domains. As noted above, the frequency distributions of QDIS-7 scores were less skewed than those of the legacy-scale scores for three of the four medical conditions studied (Fig. 2; Table 1). Therefore, using the QDIS-7 should simplify the interpretation of group-level statistics (mean, standard deviation, etc.) and of individual scores in relation to those group-level values. Figure 3 shows this study’s most important finding: The magnitude of the relationship between differences in QDIS-7 scores and differences in legacy-scale scores (i.e., the slope) was consistent across the four medical conditions studied.
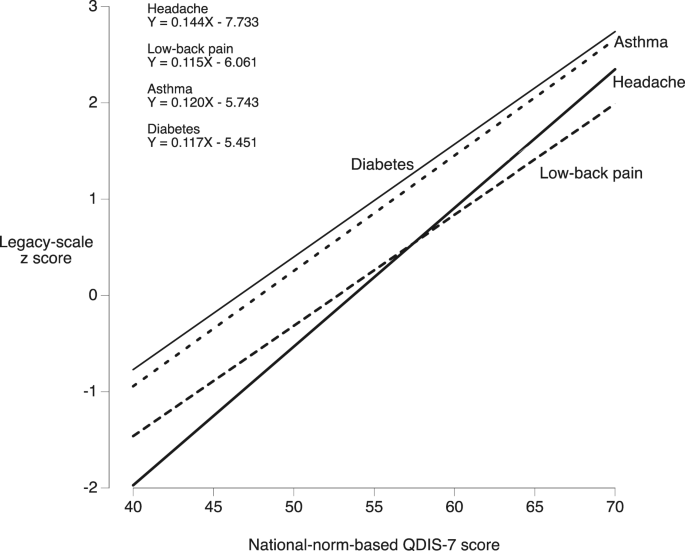
Results of regression of legacy-scale z scores on norm-based QDIS-7 scores. The slopes of the regression lines varied from 0.115 to 0.144 legacy score standard deviations per 1-point difference in norm-based QDIS-7 score. Confidence intervals of the slopes are in Table 1.
Consistency of the relation between QDIS-7 scores and legacy-scale scores across diseases (Fig. 3)
The results shown in Fig. 3 support the hypothesis posed above, that the differences in legacy scores associated with a unit difference in QDIS-7 scores (i.e., the slopes) are consistent across the four groups. In all four groups, each 10-point difference in QDIS-7 score was associated with a 1.2-to-1.4-SD difference in the score on the legacy instrument. That is, even with legacy scales of widely-varying content (Supplementary Table S2), the range over which the regression-line slopes varied was extremely small. That similarity among the four slopes has an interesting implication. It raises the possibility that a single disease-specific scale, the QDIS-7 in norm-score units, might complement or possibly in some cases be preferable to the mutually-incompatible legacy scales in their original units.
The QDIS-7 might appear to be similar to the standardized mean difference, which puts different QOL measures on a single scale20. However, as described in Supplementary Discussion S4, that similarity is superficial.
Using the QDIS-7 instead of mutually-incompatible legacy scales also facilitates comparisons of changes over time. For example, with QDIS-7 scores, a 10-point improvement caused by treatment of headache would be on the same scale as a 10-point improvement caused by treatment of asthma. Whether those two 10-point improvements justify similar clinical decisions is a separate question. Relations between QOL and clinical decisions have been addressed with different methods, such as by computing minimally important changes (MIC) for the diagnoses in question21,22, which is beyond the scope of this study.
Answering new questions
Among disease-specific QOL instruments, the QDIS-7 is uniquely useful. It allows clinicians, researchers, policy makers, etc., to answer important questions by making comparisons that were not possible previously. For example, suppose health-policy researchers compare a group of people with headache to a group with low-back pain. If those researchers are interested only in generic QOL, then they can simply use a generic instrument. But what if they are interested in disease-specific QOL? That is, what if they ask: In which of those two groups is the disease-specific impact on QOL greater? Again, such a question cannot be answered with generic QOL instruments or with legacy disease-specific QOL instruments, but it can be answered with the QDIS-7. The present study offers a concrete example: Which of the four groups had the highest disease-specific QOL and which had the lowest? And how large was the difference in disease-specific QOL between those two groups? The mean QDIS-7 scores (Table 1) show that the disease-specific impact on QOL was highest for those with low-back pain and it was lowest for those with diabetes: The mean QDIS-7 scores in those two groups were 62.6 and 46.5, respectively. (This is consistent with the fact that all people with low-back pain are symptomatic by definition, whereas some people with diabetes are asymptomatic.) That difference is 16.1 points on the QDIS-7 scale. With norm-based scoring, a difference of 10 points is 1 standard deviation, so a difference of 16.1 points is 1.61 standard deviations, which is considered to be very large23,24. This answers the two questions posed above (in italics), and it illustrates how the QDIS-7 can be used to answer questions about disease-specific QOL that previously were difficult or impossible to address.
Differential item functioning and range of applicability
Using QDIS-7 scores to compare the impacts of different conditions relies on the results of tests of differential item functioning between different conditions. Such tests have been done, and the results show that sample-specific and disease-specific scoring did not improve any of the psychometric properties of QDIS items in comparison with standardized scoring (for examples, see references7] and [25). That is, differential item functioning did not explain differences in QDIS-7 scores observed across disease conditions.
Unlike generic QOL instruments, the QDIS-7 was constructed to be used primarily with data from people who have a known diagnosis. In that sense, it is similar to legacy disease-specific instruments. Beyond that similarity, the QDIS-7 can be used to measure not only the QOL effects of any specifiable disease, but also those of almost any other namable status or condition to which an impact on QOL might be attributed. Its fill-in-the-attribution structure makes the QDIS-7 attribution-specific. Specifically, in addition to measuring the impact of diseases, the QDIS-7 may also measure the impact of symptoms (headache and low-back pain in the present study), treatments10,26, exposures27,28, and any other specifiable11 status or condition that might affect regular daily physical, psychological, or social functioning. Further testing is needed to clarify the applicability of the QDIS-7 in measuring, for example, caregivers’ QOL, healthcare workers’ QOL, maternal postpartum QOL, and QOL associated with environmental pollution27,28,29,30,31,32,33,34,35,36,37. None of those examples is a disease, but the QDIS-7 may be used to quantify the specific impact of each one on QOL, using the same metric as for asthma, diabetes, etc.
Furthermore, with new and emerging medical conditions, new disease-specific QOL instruments suddenly become needed (as during the COVID-19 pandemic29,38). Development and testing of new measures can be time-consuming and resource-intensive, but the QDIS-7 could be adapted to meet new needs quickly and easily.
Summary of the main advantage of the QDIS-7
Both the QDIS-7 and legacy disease-specific QOL measures have the advantage of being sensitive to disease-specific impacts on QOL. For legacy measures, that advantage comes with an important limitation: Impacts on QOL cannot be compared across diseases. The QDIS-7 has no such limitation. The QDIS-7’s unique advantage is that it allows quantitative comparisons of attribution-specific impacts on QOL across diseases, exposures, symptoms, treatments, etc.
Limitations, and directions for further research
First, because we conducted empirical quantitative validation tests of the QDIS-7, here we report quantitative results. Nonetheless, we look forward to qualitative studies to investigate, for example, respondents’ experiences when they attribute a QOL impact to a specific medical condition, which may yield information useful for improving the QDIS-7’s items.
Second, while the highest priority for this study was testing the QDIS-7 in relation to previously validated legacy mesasures, we recognize that further validation testing is needed. That testing should include comparisons of QDIS-7 results with results from generic health-related QOL instruments and with results from established indices of disease severity.
Third, in this study we did not address the application of the QDIS-7 to standardize attribution-specific QOL in people with more than one medical condition. While such applications can be very useful, they depend on validity with regard to discrimination between the QOL effects of different medical conditions. That is, they depend on people with multiple morbidities being able to distinguish the QOL impacts of each of their conditions. This issue of respondents’ discrimination between QOL effects of different conditions is not unique to the QDIS-7, and it is not new. In fact, all disease-specific QOL instruments assume that respondents can distinguish the influence of a specified health condition on QOL from all other influences on QOL. For example, when using the RMDQ to quantify the effect of low-back pain on QOL one must assume that people with low-back pain can distinguish the QOL impact of that condition from all other QOL impacts. That assumption of respondents’ ability to discriminate undergirds all measurement of disease-specific QOL, but it is rarely if ever mentioned, and only recently was it tested. Results of those tests show that adults most often make attributions that can distinguish the QOL impacts of each of their conditions8,9,11,25. Empirically, ratings across different aspects of QOL with attribution to a specific disease capture variance not shared with the same aspects of QOL attributed to a comorbid condition. Regarding the four medical conditions studied in the present research, evidence of respondents’ ability to discriminate has previously been reported for attributions with the following five pairs of comorbid conditions: asthma with diabetes, asthma with chronic back problems, asthma with migraine headaches, diabetes with chronic back problems, and diabetes with migraine headaches8. Furthermore, for comorbidity pairs of asthma with 22 other conditions the overall success rate of tests of discrimination was 100%8. For comorbidity pairs of diabetes with 25 other conditions, the overall success rate was 94%8. While those results are encouraging, more work directly testing the usefulness of the QDIS-7 in the presence of multimorbidity is still needed.
Fourth, we studied only four medical conditions. Those four were chosen (1) because they are commonly encountered in primary care, (2) because they are among those that have been chosen in previous studies (including our own), and (3) in anticipation of using them in future work comparing QDIS-7 scores across independent studies, and in future work comparing QDIS-7 scores across countries. They were also chosen because (4) they have been proven to substantially affect QOL (unlike, for example, hypertension), (5) each is sufficiently prevalent to enable studies of multiple conditions in the same patients for future work addressing multimorbidity, and (6) the above makes it likely that they will be focused on in comparative effectiveness research.
Fifth, another topic for future study is the comparative responsiveness of the QDIS-7, generic instruments, and legacy disease-specific instruments to changes over time12,39,40. Although the QDIS-7’s relative validity (ratio of F statistics of two different measures) can be much higher than that of a generic tool in cross-sectional comparisons7,10, definitive judgements regarding its responsiveness to change must await direct evidence from longitudinal research.
link






