
Multiple sclerosis – Diagnosis and treatment

Diagnosis
Neurological exam
Neurological exam
A complete neurological exam and medical history are needed to diagnose MS.
Multiple sclerosis FAQs
Neurologist Oliver Tobin, M.B., B.Ch., B.A.O., Ph.D., answers the most frequently asked questions about multiple sclerosis.
There are no specific tests for MS. The diagnosis is given by a combination of medical history, physical exam, MRIs and spinal tap results. A diagnosis of multiple sclerosis also involves ruling out other conditions that might produce similar symptoms. This is known as a differential diagnosis.
MRI multiple sclerosis lesions
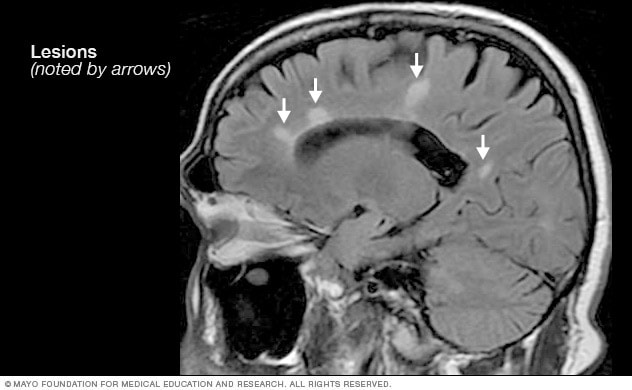
MRI multiple sclerosis lesions
Brain MRI scan showing white lesions associated with multiple sclerosis.
Lumbar puncture, also known as a spinal tap
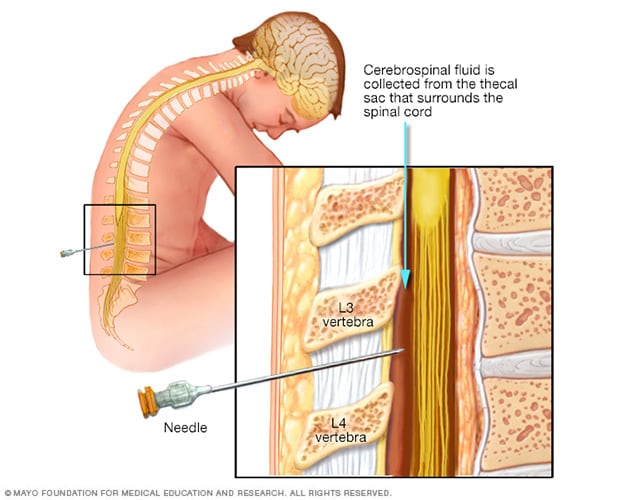
Lumbar puncture, also known as a spinal tap
During a lumbar puncture, also known as a spinal tap, you typically lie on your side with your knees drawn up to your chest. Then a needle is inserted into the spinal canal in your lower back to collect cerebrospinal fluid for testing.
Tests used to diagnose MS may include:
- MRI, which can reveal areas of MS on the brain and spinal cord. These areas are called lesions. A contrast dye may be given through an IV to highlight lesions that show the disease is in an active phase.
- Lumbar puncture, also known as a spinal tap, in which a small sample of cerebrospinal fluid is removed from the spinal canal for lab testing. This sample can show changes in antibodies that are linked to MS. A spinal tap also can help rule out infections and other conditions with symptoms similar to MS. An antibody test that looks for kappa free light chains may be faster and less expensive than previous spinal fluid tests for MS.
- Optical coherence tomography, which uses light waves to produce images of the eye. In MS, a condition called optic neuritis causes changes in the retina. Optical coherence tomography may be used to measure thickness of the retina. It also may show damage to the retinal nerve fiber.
- Evoked potential tests, which record the electrical signals produced by your nervous system in response to stimuli. An evoked potential test may use visual stimuli or electrical stimuli. In these tests, you watch a moving visual pattern, as short electrical impulses are applied to nerves in your legs or arms. Electrodes measure how quickly the information travels down your nerve pathways.
- Blood tests, which can help rule out other diseases with symptoms similar to MS. Tests to check for specific biomarkers linked to MS are being developed. These tests may help with diagnosing the disease.
- Neuropsychological testing. Neuropsychological testing involves looking at how your brain is working. Testing examines your thinking, memory, language and social skills. It also assesses your personality and mood. A psychologist with specific expertise, known as a neuropsychologist, does this testing. Neuropsychological testing is important in MS because most people with the disease have cognitive impairment. This can include memory loss and trouble with language and thinking skills that affect daily activities. Your healthcare professional may give you a baseline test soon after you are diagnosed. Then you may be retested over time.
In most people with relapsing-remitting MS, the diagnosis is straightforward. Diagnosis is based on a pattern of symptoms related to MS and confirmed by test results.
Diagnosing MS can be harder in people with unusual symptoms or progressive disease. Additional testing may be needed.

Brain MRI is often used to help diagnose multiple sclerosis.
More Information
Treatment
There is no cure for multiple sclerosis. Treatment typically focuses on speeding recovery from attacks, reducing relapses, slowing the progression of the disease and managing MS symptoms. Some people have such mild symptoms that no treatment is necessary.

Multiple sclerosis research laboratory at Mayo Clinic
Treatments for MS attacks
During an MS attack, you may be treated with:
- Corticosteroids. These medicines reduce nerve inflammation. For MS, the corticosteroids used are oral prednisone and intravenous methylprednisolone. Side effects may include insomnia, increased blood pressure, increased blood glucose levels, mood swings and fluid retention.
- Plasma exchange. This treatment involves removing the liquid part of your blood, called plasma, and separating it from your blood cells. The blood cells are then mixed with a protein solution called albumin and put back into your body. Plasma exchange may be used if your symptoms are new, severe and haven’t responded to steroids. Plasma exchange also is known as plasmapheresis.
Treatments to modify progression
There are several disease-modifying therapies (DMTs) for relapsing-remitting MS. Some of these DMTs can be of benefit for secondary-progressive MS. One is available for primary-progressive MS.
Much of the immune response linked to MS happens in the early stages of the disease. Aggressive treatment with these medicines as early as possible can lower the relapse rate and slow the formation of new lesions. These therapies may reduce the risk of lesions and worsening disability.
Many of the disease-modifying therapies used to treat MS carry serious health risks. Selecting the right therapy for you depends on many factors. Factors include how long you’ve had the disease and your symptoms. Your healthcare team also looks at whether previous MS treatments have worked and your other health issues. Cost and whether you plan on having children in the future also are factors when deciding on treatment.
Treatment options for relapsing-remitting MS include injectable, oral and infusions medicines.
Injectable treatments include:
-
Interferon beta medicines. These medicines work by interfering with diseases that attack the body. They may decrease inflammation and increase nerve growth. Interferon beta medicines are injected under the skin or into muscle. They can reduce the number of relapses and make them less severe.
Side effects of interferons may include flu-like symptoms and injection-site reactions. You’ll need blood tests to monitor your liver enzymes because liver damage is a possible side effect of interferon use. People taking interferons may develop antibodies that can reduce how well the medicine works.
- Glatiramer acetate (Copaxone, Glatopa). This medicine may help block your immune system’s attack on myelin. Glatiramer acetate is injected beneath the skin. Side effects may include skin irritation at the injection site and swelling.
- Ofatumumab (Kesimpta, Arzerra). This medicine targets cells that damage the nervous system. These cells are called B cells. Ofatumumab is given by an injection under the skin. It can decrease the risk of new lesions and new or worsening symptoms. Possible side effects are infections, local reactions to the injection site and headaches.
Oral treatments include:
- Teriflunomide (Aubagio). This once-daily oral medicine can reduce relapses. Teriflunomide can cause liver damage, hair loss and other side effects. This medicine is linked to birth defects when taken by both men and women. Use birth control when taking this medicine and for up to two years afterward. Couples who wish to become pregnant can talk to their healthcare professional about ways to remove the medicine from the body faster. Teriflunomide requires blood testing on a regular basis.
- Dimethyl fumarate (Tecfidera). This twice-daily oral medicine can reduce relapses. Side effects may include flushing, diarrhea, nausea and lowered white blood cell count. Dimethyl fumarate requires blood testing on a regular basis.
- Diroximel fumarate (Vumerity). This twice-daily capsule is similar to dimethyl fumarate but typically causes fewer side effects. It’s approved for the treatment of relapsing forms of MS.
- Monomethyl fumarate (Bafiertam) was approved by the U.S. Food and Drug Administration, also called the FDA, as a delayed release medicine that has a slow and steady action. The time release of the medication may help to decrease side effects. Possible side effects are flushing, liver damage, abdominal pain and infections.
- Fingolimod (Gilenya). This once-daily oral medicine reduces relapse rate. Your heart rate and blood pressure are monitored for six hours after the first dose because your heart rate may be slowed. Fingolimod is harmful to a developing baby. Use birth control when taking this medicine and for at least three days after stopping the medicine. Other side effects include infections that may be rare but serious, headaches, high blood pressure and blurred vision.
- Siponimod (Mayzent). This once-daily oral medicine can reduce relapse rates and help slow progression of MS. It’s also approved for secondary-progressive MS. Possible side effects include viral infections, liver damage and low white blood cell count. Other possible side effects include changes in heart rate, headaches and trouble with vision. Siponimod is harmful to a developing baby. Use birth control when taking this medicine and for at least three days after stopping the medicine. Some people need to have their heart rate and blood pressure monitored for six hours after the first dose. This medicine requires blood testing on a regular basis.
- Ozanimod (Zeposia). This once-daily oral medicine decreases the relapse rate of MS. Possible side effects are elevated blood pressure, infections and liver inflammation. Ozanimod is harmful to a developing baby. Use birth control when taking this medicine and for at least three days after stopping the medicine.
- Ponesimod (Ponvory). This oral medicine is taken once a day with a gradually increasing dosing schedule. The possible side effects are respiratory tract infections, high blood pressure, liver irritation, and changes in heart rate and rhythm. Ponesimod is harmful to a developing baby. Use birth control when taking this medicine and for at least three days after stopping the medicine.
- Cladribine (Mavenclad). This medicine is generally prescribed as a second-line treatment for those with relapsing-remitting MS. It’s also approved for secondary-progressive MS. It is given in two treatment courses, spread over a two-week period, over the course of two years. Side effects include upper respiratory infections, headaches, tumors, serious infections and reduced levels of white blood cells. People who have active long-lasting infections or cancer should not take this medicine. People who are pregnant or breastfeeding also should not take this medicine. Use birth control when taking cladribine and for the following six months. You may need blood tests on a regular basis while taking cladribine.
Infusion treatments include:
-
Natalizumab (Tysabri). This is a monoclonal antibody that has been shown to decrease relapse rates and slow down the risk of disability.
Natalizumab is designed to block the movement of potentially damaging immune cells from your bloodstream to your brain and spinal cord. It may be considered a first-line treatment for some people with relapsing-remitting MS or as a second-line treatment in others.
This medicine increases the risk of a potentially serious viral infection of the brain called progressive multifocal leukoencephalopathy (PML). Risk increases in people who are positive for antibodies that cause the PML JC virus. People who don’t have the antibodies have extremely low risk of PML.
-
Ocrelizumab (Ocrevus). This medicine is approved by the FDA to treat both the relapsing-remitting and primary-progressive forms of MS. This treatment reduces the relapse rate and the risk of disabling progression in relapsing-remitting multiple sclerosis. It also slows the progression of the primary-progressive form of multiple sclerosis.
Clinical trials showed that it reduced the relapse rate in relapsing disease and slowed worsening of disability in both forms of the disease.
Ocrelizumab is given via an IV infusion by a medical professional. Side effects may include irritation at the injection site, low blood pressure, a fever and nausea, among others. Some people may not be able to take ocrelizumab, including those with a hepatitis B infection. Ocrelizumab also may increase the risk of infections and some types of cancer, particularly breast cancer.
- Ublituximab (Briumvi). This treatment is a monoclonal antibody used to treat relapsing forms of MS. Ublituximab is given via an IV infusion while being monitored. Ublituximab may be used for people who can’t take ocrelizumab. Side effects include infusion reactions, increased risk of infections and higher risk of fetal harm.
-
Alemtuzumab (Campath, Lemtrada). This treatment is a monoclonal antibody that decreases annual relapse rates and demonstrates MRI benefits.
This medicine helps reduce relapses of MS by targeting a protein on the surface of immune cells and depleting white blood cells. This effect can limit nerve damage caused by the white blood cells. But it also increases the risk of infections and autoimmune conditions, including a high risk of thyroid autoimmune diseases and rare immune-mediated kidney disease.
Treatment with alemtuzumab involves five consecutive days of infusions followed by another three days of infusions a year later. Infusion reactions are common with alemtuzumab.
Alemtuzumab is only available from registered healthcare professionals. People treated with the medicine must be registered in a special medicine safety monitoring program. Alemtuzumab is usually recommended for those with aggressive MS or as second-line treatment if other MS medicines didn’t work.
Treatments for MS symptoms

Physical therapy for multiple sclerosis
Physical therapy can build muscle strength and ease some of the symptoms of MS.
These treatments can help relieve some of the symptoms of MS.
-
Therapy. A physical or occupational therapist can teach you stretching and strengthening exercises. The therapist also can show you how to use devices to make it easier to perform daily tasks.
Physical therapy and a mobility aid, when necessary, also can help manage leg weakness and help improve walking.
- Muscle relaxants. You may experience muscle stiffness or spasms, particularly in your legs. Muscle relaxants such as baclofen (Lioresal, Gablofen), tizanidine (Zanaflex) and cyclobenzaprine (Amrix, Fexmid) may help. Onabotulinumtoxin A (Botox) treatment is another option for muscle contractions.
- Medicines to reduce fatigue. Amantadine (Gocovri), modafinil (Provigil) and methylphenidate (Ritalin, Concerta) have been used to reduce MS-related fatigue. However, a recent study did not find these medicines to be better than a placebo in improving MS-related fatigue and caused more side effects. Some medicines used to treat depression, including fluoxetine (Prozac) and bupropion (Wellbutrin), may be recommended.
- Medicine to increase walking speed. Dalfampridine (Ampyra) may help to slightly increase walking speed in some people. Possible side effects are urinary tract infections, vertigo, insomnia and headaches. People with a history of seizures or kidney dysfunction should not take this medicine.
- Other medicines. Medicines also may be prescribed for depression, pain, sexual dysfunction, insomnia, and bladder or bowel control troubles that are linked to MS.
Recent developments or emerging therapies
Bruton’s tyrosine kinase (BTK) inhibitor is a therapy being studied in relapsing-remitting multiple sclerosis and secondary-progressive multiple sclerosis. It works by altering the function of B cells, which are immune cells in the central nervous system.
Another therapy being studied in people with MS is stem cell transplantation. This treatment destroys the immune system of someone with MS and then replaces it with transplanted healthy stem cells. Researchers are still investigating whether this therapy can decrease inflammation in people with MS and help to “reset” the immune system. Possible side effects are fever and infections.
A type of protein called CD40L found in T cells has been shown to play a role in MS. Recent studies have shown that blocking this protein can help manage MS.
A new medicine called a phosphodiesterase inhibitor also is being studied. This medicine works to reduce inflammation by changing damaging immune system responses seen in MS.
Researchers also are learning more about how existing disease-modifying therapies work to lessen relapses and reduce multiple sclerosis-related lesions in the brain. Further studies are needed to determine whether treatment can delay disability caused by the disease.
More Information
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Lifestyle and home remedies
To help relieve the symptoms of MS, try to:
- Get plenty of rest. Look at your sleep habits to make sure you’re getting the best possible sleep. If you have conditions such as obstructive sleep apnea, see a healthcare professional and get treatment.
- Exercise. If you have mild to moderate MS, regular exercise can help improve your strength, muscle tone, balance and coordination. Swimming or other water exercises are good options if heat makes your symptoms worse. Other types of mild to moderate exercise recommended for people with MS include walking, stretching, low-impact aerobics, stationary bicycling, yoga and tai chi.
- Cool down. In some people, MS symptoms may worsen as body temperature rises. It helps to stay cool and use cooling scarves or vests.
- Eat a balanced diet. Research suggests that following the Mediterranean diet may be linked to a lower risk of worsening disability in MS. The Mediterranean diet includes fruits and vegetables, whole grains, legumes, nuts, and olive oil. It also means not eating large amounts of red meats, butter, sugar and other unhealthy foods. Some research suggests that vitamin D may have potential benefit for people with MS.
- Relieve stress. Stress may trigger or worsen your symptoms. Yoga, tai chi, massage, meditation or deep breathing may help.
More Information
Alternative medicine
Many people with MS use a variety of alternative or complementary treatments to help manage their symptoms, such as fatigue and muscle pain.
Exercise, meditation, yoga, massage, eating a healthier diet, acupuncture and relaxation techniques may help boost overall mental and physical well-being.
According to guidelines from the American Academy of Neurology, research strongly indicates that oral cannabis extract (OCE) may improve symptoms of muscle contractions and pain. There is a lack of evidence that cannabis in any other form is effective in managing other MS symptoms.
Daily intake of vitamin D3 of 2,000 to 5,000 international units daily is recommended in people with MS. The connection between vitamin D and MS is supported by the association with exposure to sunlight and the risk of MS.
Coping and support
With time, you’ll find what helps you cope with the stress of a chronic illness like multiple sclerosis. Until then, you may find it helps to:
Learn enough about multiple sclerosis to make decisions about your care
Ask your healthcare team about your MS, including your test results, treatment options and, if you like, your prognosis. As you learn more about MS, you may become more confident in making treatment decisions.
Keep friends and family close
Keeping your close relationships strong can help you deal with multiple sclerosis. Friends and family can provide the practical support you may need, such as helping take care of your home if you’re in the hospital. And they can serve as emotional support when you feel overwhelmed by having MS.
Find someone to talk with
Find someone who is willing to listen to you talk about your hopes and worries. This may be a friend or family member. The concern and understanding of a counselor, medical social worker, clergy member or MS support group also may be helpful.
Preparing for your appointment
Make an appointment with a doctor or other healthcare professional if you have any symptoms that worry you.
If your healthcare professional thinks you might have multiple sclerosis, you may be referred to a doctor who specializes in conditions of the brain and nervous system, called a neurologist.
Because appointments can be brief, it’s a good idea to be prepared. Here’s some information to help you get ready.
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there’s anything you need to do in advance, such as restrict your diet.
- Write down symptoms you have, including any that may not seem related to the reason for which you scheduled the appointment.
- Write down important personal information, including major stresses or recent life changes.
- Make a list of all medicines, vitamins or supplements you’re taking and the doses.
- Take a family member or friend along. Sometimes it can be very hard to remember all the information provided during an appointment. Someone who goes with you may remember something that you missed or forgot.
- Write down questions to ask your healthcare team.
Your time with your healthcare team is limited, so preparing a list of questions can help you make the most of your time together. List your questions from most important to least important in case time runs out. For multiple sclerosis, some basic questions to ask include:
- What’s the most likely cause of my symptoms?
- What kinds of tests do I need? Do they require any special preparation?
- Is my condition likely temporary or ongoing?
- Will my condition progress?
- What treatments are available?
- I have these other health conditions. How can I best manage them together?
Don’t hesitate to ask other questions.
What to expect from your doctor
Be prepared to answer questions, such as:
- When did your symptoms begin?
- Have your symptoms been ongoing or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- Does anyone in your family have multiple sclerosis?
Nov. 01, 2024
link






