
Is mental illness really an illness?

Category: Health Published: January 8, 2024
Public Domain Image,
source: Christopher S. Baird.
Yes, mental illnesses really are physical illnesses1,2,3. Mental illnesses arise from biochemical and physical abnormalities in the brain brought on by genetic disorders, chronic medical conditions, infectious diseases such as COVID-19, traumatic brain injury, drug abuse, trauma, and other factors4,5,6. Mental illnesses are not the result of moral shortcomings, character flaws, personality weaknesses, or poor choices7,8. Abnormal neurotransmitter functioning in the brain has been found to play a large role in mental illnesses. These neurotransmitters include serotonin, dopamine, norepinephrine, glutamate, GABA, and cortisol9,10,11,12. People experiencing a mental illness did not choose their condition13 any more than people choose appendicitis or cystic fibrosis. Furthermore, people cannot find relief from a mental illness by simply choosing to be happy14 any more than people can find relief from cancer or heart disease by simply choosing to be happy.
This article was reviewed and approved by a Licensed Clinical Social Worker (LCSW) on Dec. 27, 2023. The statements in this article are based on well-established information drawn from a wide array of reputable sources that can be accessed by clicking on the numbered citation links. Furthermore, this article draws from my own experience as a licensed foster care provider, a trained advisor of university students, and a church leader.
One of the most common types of mental illness is clinical depression (i.e. major depressive disorder), so I will mainly focus on this type. One out of every twelve U.S. adults is currently having a clinical depression episode or has had one in the last year15. Clinical depression outwardly looks similar to a healthy person having a bad day. However, the causes are different, the suffering is different, and the prognosis is different16. Because clinical depression and normal sadness outwardly look similar, it can be tempting for people to assume that they are the same, which leads them to treat someone with clinical depression unfairly, unhelpfully, and illogically.
How is clinical depression different from normal sadness?
People who are experiencing normal sadness can cheer themselves up by doing uplifting activities that they enjoy. If these people view clinical depression and normal sadness as the same, they will be tempted to see people with depression as weak-willed individuals who need to try harder to cheer themselves up. This viewpoint is incorrect and unfair17. That’s like seeing a person with diabetes as weak because he can’t cure his diabetes through happy thoughts. Well-meaning friends and family may say, “When I’m feeling down, I watch a happy movie and it makes me feel better – why can’t you do that?” If watching a happy movie drives away their sadness, then they don’t have clinical depression18, so their insights about how to deal with sadness are unrelated and unhelpful.
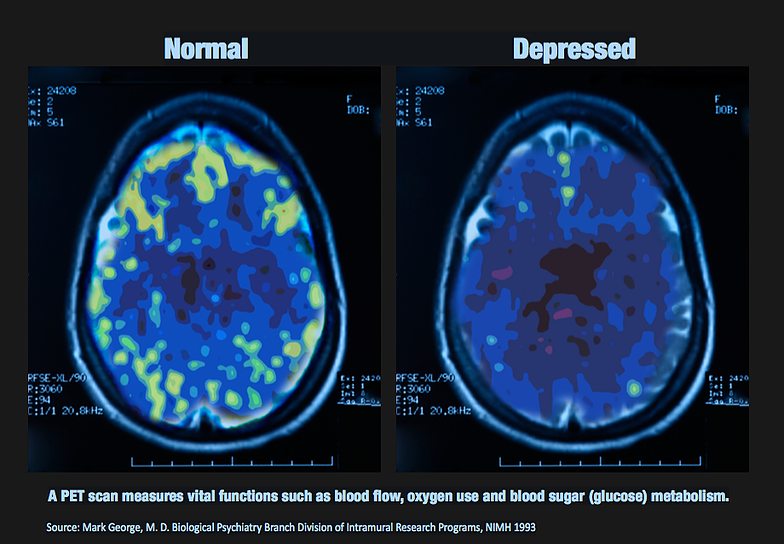
PET brain scans. Click to enlarge. Public Domain Image, source: Mark George, NIMH.
People with normal sadness can cheer themselves up by playing a sport, doing art, playing a game, eating ice cream, watching a fun show, visiting a friend, listening to music, doing service, repeating inspiring quotes, and so forth. People experiencing clinical depression can’t. Period. It’s not that those with clinical depression are too lazy or too weak to cheer themselves up, or that they don’t want to be cheered up. Rather, they are physically incapable of cheering themselves up19. The biochemical and physical abnormalities in their brains won’t allow it. A person experiencing clinical depression may try to watch a fun movie, and want it to cheer him up, and try hard to let it cheer him up, and know that others are cheered up by this movie, and yet… it doesn’t help him. This realization then adds to the sadness. It’s like realizing that everyone else can experience the wonderful taste of chocolate except for you. The sight of chocolate then makes you sad because it reminds you that you can’t taste it. In this way, enjoyable activities can do more harm than good, so that the person with depression begins avoiding them20. If you are trying to help a friend or loved one who is experiencing clinical depression, it is counterproductive to encourage him or her to do an enjoyable activity to cheer up. Well-meaning statements such as, “You should listen to fun music more – then you’ll be happy,” are false and unhelpful. Furthermore, such statements can be hurtful because they incorrectly imply that the root problem is laziness or weakness.
Why are people with depression sad even if they have a great life?
Well-meaning friends and family may say to a person experiencing clinical depression, “Why are you so sad all the time? You have a great life. You have no reason to be sad.” The truth is, being sad for extended periods of time for no apparent reason is what it means to have clinical depression21 (in most cases). Biochemical and physical abnormalities in the brain force people with clinical depression to experience incredibly real sadness and incredibly overwhelming hopelessness for no reason. The realization of this fact can be infuriating for the sufferer, which makes the depression worse. The abnormalities in the brain cause the sadness and hopelessness to feel painfully real and convincingly justified. The person can’t just tell himself, “Being sad is nonsense because I have a great life,” and then make the sadness go away. If you are trying to help a friend or loved one who is experiencing clinical depression, it is unhelpful and counterproductive to tell him that he shouldn’t be sad because he has no reason to be sad.
Does depression cause more than sadness?
Yes. Because clinical depression is an illness, it causes more problems than sadness and hopelessness. People with clinical depression also typically experience memory loss, concentration problems, sleep disturbances, back pain, headaches, and a lack of energy22,23. These other problems are direct physical results of the illness itself and are not by-products of poor choices, a bad attitude, or an inability to cope. You often hear about the sadness that comes from clinical depression, but you don’t often hear about these other problems. However, for many people, these other problems significantly contribute to their suffering, disrupting their ability to carry out work responsibilities, build relationships, be involved in the community, and even carry out the basic functions of life24. Just like how people experiencing clinical depression cannot wish away the sadness, it should be obvious that they also cannot wish away the memory loss, back pain, and other problems.
Can people with depression find relief?
Fortunately, because clinical depression involves biochemical neurotransmitter abnormalities in the brain, it can often be successfully treated using medication that affects these neurotransmitters, as well as by using therapies that rewire the brain. Most people who have clinical depression eventually find complete relief, or partial but significant relief, using psychotropic medications and therapy. The National Institute of Mental Health conducted a large-scale study using a sequenced, adaptive treatment approach and found that 70% of the people in the study who had experienced clinical depression and had carried out the entire treatment sequence eventually reached full remission and found complete relief, thanks to targeted medication and therapy25. To be clear, medications and therapies do not cure the depression. Rather, as long as people continue to use the medications and therapies that help them, most people with clinical depression eventually find complete relief, or partial but significant relief, and are able to live enjoyable, productive, fulfilling lives26. This is somewhat similar to how there is no cure for diabetes, but most people with diabetes who consistently receive proper treatment and regulate their food consumption are able to eliminate or minimize their symptoms. Amazingly, because the memory loss, concentration problems, sleep disturbances, back pain, headaches, and lack of energy resulted from the illness, a medication that successfully drives away most of the sadness will often also successfully drive away most of these other problems.
What are unhelpful things to say to a friend or loved one experiencing clinical depression?
- You have a great life. You have no reason to be sad.
- Your problems aren’t as big as you think.
- My life is way harder than yours, and I’m still happy. What’s your problem?
- Your attitude is selfish. I have problems too.
- I’m far too busy with my own problems to care about your imaginary problems.
- I have too much going on to worry about your feelings.
- You’re thinking about yourself too much.
- It’s all in your head. You should focus on the real world.
- Just snap out of it.
- Just focus on the positive things in your life.
- You just need to count your blessings.
- You should be grateful for what you have.
- It could be worse.
- You should pray more and have more faith.
- Have you ever tried not being depressed?
- Try harder to cheer yourself up.
- Raw willpower does the job. Toughen up.
- You should make more of an effort to not be so lazy and weak.
- Getting things done is more important than feelings.
- Don’t cry. It makes you look weak.
- You’re not the type of person to be depressed.
- I don’t think you really have depression. You look fine to me.
- It can’t be that bad. You look happy at parties.
- You’re imagining things.
- This too shall pass.
- You’ll get over it.
- I know how you feel.
- Watching a happy movie always cheers me up. You should try that.
- You should listen to music that is more uplifting and inspiring.
- A good workout will make you feel better. It works for me.
- You don’t need medication. I can pull myself out of sadness without needing medication. Why can’t you?
- Using medication is giving up and running away from your problems.
- You used to love painting landscapes. Why don’t you do that more?
- Try cooking yourself a treat.
- You just need a good book to read.
- Go play with your dog more.
- Have you tried essential oils?
- You’ll feel better if you connect with nature – go hiking or canoeing.
- You just need to get into a good TV series.
- You’ll forget about your problems if you get out more.
- Do some community service – then your problems won’t seem so bad.
- Let me read to you this inspiring quote. It will help you.
- This sermon from church is so encouraging. You should read it.
- Just get busy with work and you won’t have time for self-pity.
What are helpful things to say to a friend or loved one experiencing clinical depression?
- How do you feel right now? (And then you simply listen without giving any advice.)
- Keep talking. I’m listening.
- I am sorry that you are suffering.
- I don’t know what to say, but I’ll sit here with you.
- It’s okay to cry. I’ll stay here with you.
- I care about you.
- Your feelings are valid. Your suffering is real.
- I am sorry you are hurting so much. It must be hard.
- I am here for you. I support you.
- You’re not going crazy, but it probably feels like that.
- What errands can I run for you? Do you need groceries?
- Do you have any medications that need to be picked up?
- Would you like me to set up an appointment for you with a doctor? or therapist? or nurse practitioner?
- Would it be helpful if I come with you to your doctor appointment? or therapist appointment? or nurse practitioner appointment?
- Are you getting the care that you need from your doctors, therapists, and nurse practitioners? I can help you find alternatives if need be.
- You probably need some professional medical help. If you don’t already have one that you are working with, I can find a doctor for you, or a therapist, or a nurse practitioner.
- Are you considering hurting yourself or ending your life?
If the person firmly answers “yes” to the last question, immediately call the suicide hotline, which is “988” in the United States27. You may need to immediately drive your loved one to a psychiatric hospital or a general-purpose hospital. Stay with your loved one until he or she can be professionally assessed. If the person poses an immediate threat28 to you or to himself/herself, immediately call 911 in North America, 112 in Europe, or your country’s emergency number.
Are mental illnesses common?
Yes, mental illnesses are common. One in five adults in the U.S. are currently experiencing a mental illness or have experienced a mental illness in the past year29. If you go to a party with twenty adults, typically four people at the party are experiencing or have recently experienced a mental illness. If you sit in a church service with two hundred adults in the congregation, typically forty of them are experiencing or have recently experienced a mental illness.
People don’t like talking about mental illnesses, so they seem much less common than they actually are. Furthermore, mental illnesses affect people from all walks of life. If you were sitting at a meeting at work and could magically see an arrow hovering over every person that is experiencing or has recently experienced a mental illness, you would likely be surprised by who it is. Humorous people experience mental illness. Highly successful people experience mental illness. Women, men, black, white, young, old, athletes, poets, artists, engineers, lawyers, doctors, scientists, plumbers, and farmers all experience mental illness30.
Considering that mental illnesses are so common, everyone should become more informed about them, be more open to talking about them, and look for opportunities to support others who are affected. For every ten of your friends and relatives, typically two of them are experiencing or have recently experienced a mental illness, whether you know it or not.
Are people with a mental illness weak?
No, people with a mental illness are not weak31. Once you learn what mental illness really is, and interact closely with a dear friend or family member who has a mental illness, you will come to realize how amazingly strong he or she is. For a person with clinical depression or an anxiety disorder, getting out of bed, getting dressed, and going to a doctor will likely require more emotional and mental strength than what many people will have to muster all year. For people suffering from a mental illness, seeking out and using medication is a sign of strength, not a sign of weakness. It signifies that they have the strength to face their illness and the courage to deal with it. It signifies that they are moving forward along the path toward relief and remission. Taking prescription medication for a mental illness is no more a sign of weakness than a person taking insulin for diabetes. Receiving therapy for a mental illness is no more a sign of weakness than a person with a broken arm getting a cast. Although “therapy” is often a punchline in movies, it can be life-saving and life-changing in the real world. When a person with a mental illness is willing to try a prescribed medication or an evidence-based therapy, it is a success. Mental illness is not a normal part of life that people should ignore.
Are people with a mental illness crazy or dangerous?
The majority of people with a mental illness are not crazy or dangerous32. Most people with a mental illness do not think they are Napoleon, do not experience hallucinations, and do not pose a threat. The large majority of the people around you with a mental illness are not criminals or mass murderers. Most people experiencing a mental illness do not act frighteningly bizarre in public33. In fact, because of the prevalent negative stigma associated with mental illnesses, many people with a mental illness try to hide it. Such people put on a false happy or calm face in public, so that they are indistinguishable from others in public. The bottom line is that acquaintances, relatives, and friends do not need to be nervous, awkward, creeped out, or on their guard when around people with a mental illness.
When a person goes to a psychiatric hospital or to the psychiatric ward of a general-purpose hospital, it is a sign of strength and hope. In modern times, a psychiatric hospital is not a place where crazy people are pointlessly and endlessly locked away, hidden from the view of society. Rather, a psychiatric hospital is a place where regular people who are experiencing severe illness can find treatment, relief, and improvement34. When people go to a psychiatric hospital, clinic, or ward for treatment, it is a success. It means that he or she is moving forward along the path toward relief and remission.
A person going to a psychiatric hospital, clinic, or ward for treatment is no stranger than a person with kidney failure going to a hospital or clinic for treatment. Sadly, movies and television often portray people with a mental illness as crazy, creepy, evil, or amusingly quirky. For the large majority of people, this is far from the truth. In the real world, mental illness involves suffering and impairment. Mental illnesses are not intriguing, cute, amusing, quirky, or funny. Our loved ones with a mental illness deserve our empathy, understanding, patience, respect, and support; not our platitudes, avoidance, awkwardness, or cartoonish stereotypes.
Why do antidepressant medications take so long to be beneficial?
A person with clinical depression has more physically wrong with his or her brain than having incorrect levels of neurotransmitters. The science in this area is not completely understood, but the illness likely also involves neurons becoming desensitized to neurotransmitters35, abnormally small brain areas36, and irregular neural pathways37. A psychotropic medication may be able to normalize neurotransmitter levels within days, but it still takes time for the neurons to become properly sensitized again and for the neural pathways to be rewired properly. For most people with clinical depression, it will take from one to two weeks of taking an effective psychotropic medication before seeing any benefit at all, and will take three months or more of taking the medication before reaching the maximum benefit38. This should not be surprising if you keep in mind that a broken bone takes months to heal.
For a person with clinical depression who has found a medication that works for him or her, there is gradual but meaningful improvement over the following weeks and months. However, the “gradual but meaningful improvement” does not typically mean that there is steady, smooth improvement. Rather, there can still be fluctuations between hard days and good days, while the long-term average shows continual, meaningful improvement. For this reason, a person on a psychotropic medication should not give up on the medication upon having a hard day, thinking that the medication is not working. (Also, a person should not stop taking a psychotropic medication without first getting approval from the prescribing doctor or nurse practitioner because there can be serious withdrawal symptoms39.)
Is depression just a behavioral illness?
No. Clinical depression is much more than just a behavioral illness40. Acquaintances, family, and friends can only see the outward abnormal behaviors that result from someone experiencing clinical depression and therefore may assume… that’s all there is. However, clinical depression also involves intense inner suffering. A person could successfully hide this inner suffering and act normal, so that there would be no outward behavioral abnormalities. However, the suffering is still real, whether it leads to noticeable behavioral problems or not. Clinical depression is more than an emotional illness or a mood disorder. It often includes memory loss, lack of concentration, headaches, body aches, slowed mental processing, and disorganized thought41; all things that are not directly related to emotions. These problems arise physically from the illness itself and not from the expression of a bad mood. Clinical depression is a brain illness that can cause significant physical, mental, cognitive, emotional, and behavioral impairment and suffering. The goal of treatment is to relieve all of these facets of the illness, and not just to normalize outward behaviors.
Do antidepressants change someone’s personality?
No. Antidepressants do not change a person’s personality42. For an antidepressant that is working for a particular person, the most common result is that the person feels more like his normal, original, true self. In other words, effective antidepressants let a person’s true personality shine through again, instead of being locked up in mental prison.
Is there one antidepressant medication that works for everyone?
No. The human brain is incredibly complex and diverse. There are many different forms of depression and people respond to the same medication in many different ways. For this reason, there are many different types of medication. One particular medication may significantly help many people but give no benefit to other people, while other particular medications may significantly help the other people but give no benefit to the first people43. Sometimes a combination of medications brings relief and improvement. For these reasons, people with clinical depression typically do not see any benefit from the first medication that they try, but then find benefit from other medications44. It usually takes trying different medications, one after the other, until a person finds a medication that helps him or her. Because it can takes months to tell whether a particular antidepressant medication is helping or not, this process can take several months or even years.
If you have a friend or loved one experiencing a mental illness who has tried one medication that ended up not helping and then gave up on medications entirely, you should encourage him or her to keep going back to the medical professionals and keep trying other medications. For many people, a combination of medication and therapy gives the maximum benefit. Effective therapies for clinical depression include biofeedback, cognitive behavioral therapy (CBT), group therapy, and other talk therapies45,46. Regular exercise can also be beneficial for many people, especially if used in conjunction with medication and therapy47.
How can a person tell if he has clinical depression or just typical sadness?
Primary care physicians can quickly assess a person for clinical depression48 and determine if he or she needs further assessment, should see a psychiatrist, or should start taking a medication. If you have a family member or friend who is showing signs of clinical depression, encourage him or her to go to the doctor and get assessed. If it is appropriate for your relationship, offer to make the doctor’s appointment and go with him or her to the appointment. In short, the best way to tell if sadness is clinical depression is to go to the doctor for a professional assessment. In addition to primary care physicians, psychiatrists and psychiatric-mental health nurse practitioners can also perform professional assessments of mental illness.
Warning signs of clinical depression include49: comments about self-harm or not wanting to live, sadness or hopelessness that lasts more than two weeks, a loss of interest in the hobbies and projects that the person used to enjoy, ongoing sleep problems, and mental or emotional problems that are disrupting work, relationships, or the basic chores of everyday life. Note that clinical depression can be very different from one person to the next and may not exactly match these descriptions. Also, there are many other mental illnesses besides depression that I have not specifically talked about much in this article, but may require your closer attention.
The good news is that there is hope! The majority of people with a mental illness eventually find complete relief, or partial but significant relief, after determining the right medication, finding the right therapies, and allowing enough time to pass for the healing process to work50.
SOURCES
1. American Psychiatric Association: “What is Mental Illness?” (Reviewed 2022).
https://www.psychiatry.org/patients-families/what-is-mental-illness
2. University of Rochester Medical Center, Health Encyclopedia: “What You Need to Know About Mental Illness.”
https://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=1&ContentID=3047
3. National Alliance on Mental Illness (NAMI): “Dispelling Myths on Mental Illness” by Sarah Powell (2015).
https://www.nami.org/Blogs/NAMI-Blog/July-2015/Dispelling-Myths-on-Mental-Illness
4. Mayo Clinic: “Mental Illness” (2022).
https://www.mayoclinic.org/diseases-conditions/mental-illness/symptoms-causes/syc-20374968
5. Cleveland Clinic: “Mental Health Disorders” (Reviewed 2022).
https://my.clevelandclinic.org/health/diseases/22295-mental-health-disorders
6. Biological Psychiatry: “Depression, Hypothalamic Pituitary Adrenal Axis, and Hippocampal and Entorhinal Cortex Volumes—The SMART Medea Study” by Lotte Gerritsen, et. al. (2011).
https://pubmed.ncbi.nlm.nih.gov/21439552/
7. Substance Abuse and Mental Health Services Administration (SAMHSA): “Mental Health Myths and Facts” (2023).
https://www.samhsa.gov/mental-health/myths-and-facts
8. National Alliance on Mental Illness (NAMI): “Dispelling Myths on Mental Illness” by Sarah Powell (2015).
https://www.nami.org/Blogs/NAMI-Blog/July-2015/Dispelling-Myths-on-Mental-Illness
9. National Institutes of Health, Biological Sciences Curriculum Study: “Information about Mental Illness and the Brain” (2007).
https://www.ncbi.nlm.nih.gov/books/NBK20369/
10. Landmark Papers in Psychiatry: “Chapter 3. The neurochemical basis of psychiatric disorders” by Elizabeth Ryznar and Herbert Y. Meltzer (2020).
https://academic.oup.com/book/29852/chapter-abstract/252984421
11. The Journal of Clinical Psychiatry: “Neurotransmitter Targeting in the Treatment of Depression” by Pierre Blier (2013).
https://www.psychiatrist.com/jcp/neurotransmitter-targeting-treatment-depression/
12. Translational Psychiatry: “Diagnosis of major depressive disorder based on changes in multiple plasma neurotransmitters: a targeted metabolomics study” by Jun-Xi Pan, et. al. (2018).
https://www.nature.com/articles/s41398-018-0183-x
13. Mental Health Literacy: “Mental Disorders.”
https://mentalhealthliteracy.org/mental-disorders/
14. NYC Psychiatric Associates: “Mental Health Myths and Facts.”
https://nycpsychiatricassociates.com/blog/mental-health-myths-and-facts/
15. National Alliance on Mental Illness (NAMI): “Mental Health By the Numbers” (2023).
https://www.nami.org/mhstats
16. National Institute of Mental Health, Fact Sheet: “Depression in Women: 5 Things You Should Know” (2020).
https://www.nimh.nih.gov/health/publications/depression-in-women
17. National Institute of Mental Health, Fact Sheet: “Depression in Women: 5 Things You Should Know” (2020).
https://www.nimh.nih.gov/health/publications/depression-in-women
18. Colby College, CogBlog: “When ‘Just Cheering Up’ Isn’t Possible” by Emily Riley (2020).
https://web.colby.edu/cogblog/2020/12/07/when-just-cheering-up-isnt-possible-the-cognitions-behind-depression-may-be-the-key-to-ending-misconceptions/
19. WebMD: “Dealing With the Stigma of Major Depressive Disorder” by Sonja Wasden (Reviewed 2023).
https://www.webmd.com/depression/features/mdd-stigma
20. Mayo Clinic: “Depression (major depressive disorder).”
https://www.mayoclinic.org/diseases-conditions/depression/symptoms-causes/syc-20356007
21. Talkiatry: “What does depression feel like?” by Wendi Waits (2023).
https://www.talkiatry.com/blog/what-does-depression-feel-like
22. Mayo Clinic: “Clinical depression: What does that mean?” by Daniel K. Hall-Flavin (2017).
https://www.mayoclinic.org/diseases-conditions/depression/expert-answers/clinical-depression/faq-20057770
23. Medical News Today: “Are depression and memory loss connected?” by Zawn Villines (Reviewed 2023).
https://www.medicalnewstoday.com/articles/depression-and-memory-loss
24. WebMD: “Untreated Depression” by Debra Fulghum Bruce (Reviewed 2021).
https://www.webmd.com/depression/untreated-depression-effects
25. Cleveland Clinic Journal of Medicine: “The STAR*D study: Treating depression in the real world” by Bradley N. Gaynes, et. al. (2008).
https://www.ccjm.org/content/ccjom/75/1/57.full.pdf
26. Cleveland Clinic Journal of Medicine: “The STAR*D study: Treating depression in the real world” by Bradley N. Gaynes, et. al. (2008).
https://www.ccjm.org/content/ccjom/75/1/57.full.pdf
27. 988 Suicide & Crisis Lifeline.
https://988lifeline.org/
28. Medical News Today: “What to know about suicidal depression” by Jenna Fletcher (Reviewed 2023).
https://www.medicalnewstoday.com/articles/suicidal-depression
29. National Alliance on Mental Illness (NAMI): “Mental Health By the Numbers” (2023).
https://www.nami.org/mhstats
30. National Alliance on Mental Illness (NAMI): “Mental Health By the Numbers” (2023).
https://www.nami.org/mhstats
31. Substance Abuse and Mental Health Services Administration (SAMHSA): “Mental Health Myths and Facts” (2023).
https://www.samhsa.gov/mental-health/myths-and-facts
32. Substance Abuse and Mental Health Services Administration (SAMHSA): “Mental Health Myths and Facts” (2023).
https://www.samhsa.gov/mental-health/myths-and-facts
33. ICJIA Research: “Mental Illness and Violence: Is there a Link?” by Emilee Green (2020).
https://icjia.illinois.gov/researchhub/articles/mental-illness-and-violence-is-there-a-link/
34. La Amistad Behavioral Health Services: “Breaking Common Myths About Mental Health Hospitals” (2022).
https://lamistad.com/blog/breaking-common-myths-about-mental-health-hospitals/
35. ACS Chemical Neuroscience: “Delayed Antidepressant Efficacy and the Desensitization Hypothesis” by Kathryn G. Commons and Sofia E. Linnros (2019).
https://pubs.acs.org/doi/10.1021/acschemneuro.8b00698
36. American Journal of Psychiatry: “Hippocampal Volume and Depression: A Meta-Analysis of MRI Studies” by Poul Videbech and Barbara Ravnkilde (2015).
https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.161.11.1957
37. Journal of Psychiatry & Neuroscience: “Adult neuroplasticity: A new “cure” for major depression?” by Paul R. Albert (2019).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6488487/
38. Cleveland Clinic: “Clinical Depression (Major Depressive Disorder)” (Reviewed 2022).
https://my.clevelandclinic.org/health/diseases/24481-clinical-depression-major-depressive-disorder
39. Mayo Clinic: “Antidepressants: Selecting one that’s right for you” (2022).
https://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20046273
40. Johns Hopkins Medicine: “Major Depression.”
https://www.hopkinsmedicine.org/health/conditions-and-diseases/major-depression
41. Johns Hopkins Medicine: “Major Depression.”
https://www.hopkinsmedicine.org/health/conditions-and-diseases/major-depression
42. WebMD: “Fears and Facts About Antidepressants” by Mary Anne Dunkin (Reviewed 2023).
https://www.webmd.com/depression/fears-and-facts-about-antidepressants
43. Cleveland Clinic: “Antidepressants” (Reviewed 2023).
https://my.clevelandclinic.org/health/treatments/9301-antidepressants-depression-medication
44. Mayo Clinic: “Antidepressants: Selecting one that’s right for you” (2022).
https://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20046273
45. Healthline: “Everything You Need to Know About Depression (Major Depressive Disorder)” by Valencia Higuera (Reviewed 2023).
https://www.healthline.com/health/depression
46. Cleveland Clinic: “Biofeedback” (Reviewed 2023).
https://my.clevelandclinic.org/health/treatments/13354-biofeedback
47. Frontiers in Pharmacology: “Is the Comparison between Exercise and Pharmacologic Treatment of Depression in the Clinical Practice Guideline of the American College of Physicians Evidence-Based?” by Yael Netz (2017).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5430071/
48. The Primary Care Companion to the Journal of Clinical Psychiatry: “Depression: Diagnosis and Management for the Primary Care Physician” by James M. Ferguson (2000).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC181135/
49. National Institute of Mental Health: “Depression” (Reviewed 2023).
https://www.nimh.nih.gov/health/topics/depression
50. Substance Abuse and Mental Health Services Administration (SAMHA): “Recovery from Substance Use and Mental Health Problems Among Adults in the United States” (2023).
https://store.samhsa.gov/sites/default/files/pep23-10-00-001.pdf
If you liked my explanation, then you’ll love my new book: The Top 50 Science Questions with Surprising Answers. Check it out! This book has been years in the making, but it’s finally available. It contains detailed, highly accurate, surprising answers to science questions like this one that you just read. It includes a substantial amount of original content that can only be found in the book.
link






